LUMBAR DISC DISEASE
By Dr.Prasanth
Kerala Ayurveda Hospital
-Pain
-Radiculopathy
-Severity
-Chronicity
-Numbness/burning/tingling and other neurological symptoms
-Pain upon coughing/sneezing
-Pain upon sitting/standing/walking
-Wether pain present upon rest
-Wether morning stiffness present or not
-Any history of RTA/TRAUMA
-Any history of LAMINECTOMY/DISCECTOMY
-Any history of chronic physical strain
-Any history of continuous travelling esp in two wheeler
-Any history of sitting before computer
-Other relevant occupational history
-XRAY/MRI/NEURO
REPORT/DOPPLER/CT SCAN ???
SLR
The straight
leg raise, also called Lasègue's sign, Lasègue test or Lazarević's sign,
is a test done during the physical examination to determine whether a patient
with low back pain has an underlying herniated disk,
often located at L5 (fifth lumbar spinal nerve).
With the patient lying down on
his or her back on an examination table or exam floor, the examiner lifts the
patient's leg while the knee is straight.
A
variation is to lift the leg while the patient is sitting.[1] However,
this reduces the sensitivity of the test.
If the patient experiences sciatic pain when
the straight leg is at an angle of between 30 and 70 degrees, then the test is
positive and a herniated disc is likely to be the cause of the pain.
A meta-analysis reported the accuracy as:
·
sensitivity 91%
·
specificity 26%
If
raising the opposite leg causes pain (cross or contralateral straight leg
raising):
·
sensitivity 29%
·
specificity 88%
Lasègue's sign was named
after Charles Lasègue (1816-1883). In
1864 Lasègue described the signs of developing low back pain while
straightening the knee when the leg has already been lifted. In 1880 Serbian
doctor Laza Lazarević described the straight leg raise test as it is used today, so the sign
is often named Lazarević's sign in Serbia and some other countries.
Gait
The pattern of how a
person walks is called the gait. Different types of walking problems occur
without a person's control. Most, but not all, are due to a physical
condition.
Some walking
abnormalities have been given names:
- Propulsive gait -- a stooped,
stiff posture with the head and neck bent forward
- Scissors gait -- legs flexed
slightly at the hips and knees like crouching, with the knees and thighs
hitting or crossing in a scissors-like movement
- Spastic gait -- a stiff,
foot-dragging walk caused by a long muscle contraction on one side
- Steppage gait -- foot drop
where the foot hangs with the toes pointing down, causing the toes to
scrape the ground while walking, requiring someone to lift the leg higher
than normal when walking
- Waddling gait -- a duck-like
walk that may appear in childhood or later in life
Abnormal gait may be caused by
diseases in many different areas of the body.
General causes of abnormal gait may include:
- Arthritis of the leg or foot joints
- Conversion disorder (a psychological disorder)
- Foot
problems (such as a callus, corn, ingrown toenail, wart, pain, skin sore,
swelling, or spasms)
- Fracture
- Injections
into muscles that causes soreness in the leg or buttocks
- Infection
- Injury
- Legs
that are different lengths
- Myositis
- Shin
splints
- Shoe
problems
- Tendonitis
- Torsion of the testis
This list does not include all causes of abnormal gait.
CAUSES OF SPECIFIC GAITS
- Propulsive
gait:
- Carbon monoxide
poisoning
- Manganese
poisoning
- Parkinson's disease
- Use
of certain drugs including phenothiazines, haloperidol, thiothixene,
loxapine, and metoclopramide (usually drug effects are temporary)
- Spastic
(scissors) gait:
- Brain abscess
- Brain or head trauma
- Brain tumor
- Cerebrovascular
accident (stroke)
- Cerebral palsy
- Cervical spondylosis with myelopathy (a problem with
the vertebrae in the neck)
- Liver
failure
- Multiple sclerosis
- Pernicious anemia
- Spinal cord trauma
- Spinal
cord tumor
- Syphilitic
meningomyelitis
- Syringomyelia
- Steppage
gait:
- Guillain-Barre syndrome
- Herniated
lumbar disk
- Multiple
sclerosis
- Muscle
weakness of the tibia
- Peroneal neuropathy
- Poliomyelitis
- Spinal
cord injury
- Waddling
gait:
- Congenital hip
dysplasia
- Muscular dystrophy
- Muscle
disease (myopathy)
- Spinal muscle atrophy
- Ataxic
or broad-based gait
- Acute cerebellar ataxia
- Alcohol
intoxication
- Brain
injury
- Damage
to nerve cells in the cerebellum of the brain (cerebellar degeneration)
- Medications
(phenytoin and other seizure medications)
- Polyneuropathy
(damage to many nerves, as occurs with diabetes)
- Stroke
Treating the cause
often improves the gait. For example, gait abnormalities from trauma to part of
the leg will improve as the leg heals.
Physical therapy
almost always helps with short-term or long-term gait disorders. Therapy will
reduce the risk of falls and other injuries.
For an abnormal gait
that occurs with conversion disorder, counseling and support from family
members are strongly recommended.
For a propulsive gait:
- Encourage the person to be as
independent as possible.
- Allow plenty of time for daily
activities, especially walking. People with this problem are likely to
fall because they have poor balance and are always trying to catch up.
- Provide walking assistance for
safety reasons, especially on uneven ground.
- See a physical therapist for
exercise therapy and walking retraining.
For a scissors gait:
- People with a scissors gait
often lose skin sensation. Skin care should be used to avoid skin sores.
- Leg braces and in-shoe splints
can help keep the foot in the right position for standing and walking. A
physical therapist can supply these and provide exercise therapy, if
needed.
- Medications (muscle relaxers,
anti-spasticity medications) can reduce the muscle overactivity.
For a spastic gait:
- Exercises are encouraged.
- Leg braces and in-shoe splints
can help keep the foot in the right position for standing and walking. A
physical therapist can supply these and provide exercise therapy, if
needed.
- A cane or a walker is
recommended for those with poor balance.
- Medications (muscle relaxers,
anti-spasticity medications) can reduce the muscle overactivity.
For a steppage gait:
- Get enough rest. Fatigue can
often cause a person to stub a toe and fall.
- Leg braces and in-shoe splints
can help keep the foot in the right position for standing and walking. A
physical therapist can supply these and provide exercise therapy, if
needed.
For a waddling gait,
follow the treatment your health care provider prescribed.
Tenderness graded as from +ve
to ++++ve
tenderness is pain or discomfort when an affected area is touched. it should not be confused with pain.
Pain is patient's perception; while tenderness is a sign thatclinician elicits.
+ve for
Slight or mild tolerable discomfort on
palpation
++ve for More
severe pain on ordinary palpation, which the patient prefers not to tolerate
+++ve for More intolerable pain even with light
palpation or pressure
++++ve for Pain
which may be caused by even a mild stimulus such as a sheet touching the joint
often characteristic of acute gout
Swelling graded as from +ve to ++++ve
swelling, turgescence or tumefaction is
a transient abnormal enlargement of a body part or area not caused by proliferation of cells.It
is caused by accumulation of fluid in tissues. It can occur throughout the body
(generalized), or a specific part or organ can be affected (localized).
+Ve for Join swelling which may not be apparent on
casual inspection, but should be recognizable to an experienced examiner
++ve for Joint
swelling obvious even on casual observation
+++ve for Markedly
abnormal swelling
++++ve for Joint
swelling to a maximally abnormal degree
Limitation of motion ranging
from 0 to 100%
About 25% loss of motion
About 50% loss of motion
About 75% loss of motion
About 75% loss of motion
100% loss of motion or complete
ankyloses of the joint
DTR
:
Patient
should be relaxed and positioned symmetrically, preferably lying supine.Biceps reflex: (C5-C6) With the arm gently flexed at the elbow, tap the biceps tendon with a reflex hammer. It may help to locate this tendon with your thumb, and strike your own thumb with the hammer. There should be a reflex contraction of the biceps brachii muscle (elbow flexion).
{kind=link}
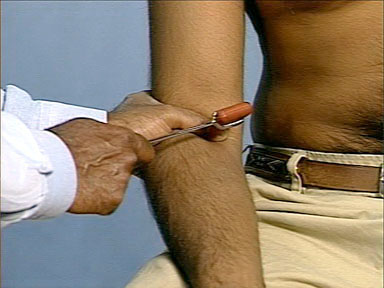
Triceps reflex: (C7-C8) With the elbow in flexion, tap the triceps tendon, just proximal to the elbow, with a reflex hammer. The arm could also be abducted at the shoulder for this maneuver. There should be a reflex contraction of the triceps muscle (elbow extension).
Brachiradialis reflex: (C5-C6)
Knee reflex: (L2-L4) Slightly lift up the leg under the knee, and tap the patellar tendon with a reflex hammer. There should be a reflex contraction of the quadriceps muscle (knee extension). (If performed in a sitting position, have the legs dangle over the edge of the chair or table).
Ankle reflex: (S1) Slightly externally rotate at the hip, and gently dorsiflex the foot, tapping the Achilles tendon with a reflex hammer. There should be a reflex contraction of the gastrocnemius muscle (plantar flexion).
When the reflexes are absent try eliciting it after re-enforcing (Jendrassik maneuver0, by asking the patient to interlock and pull flexed fingers.
Deep tendon reflexes should be graded on a scale of 0-4 as follows:
0 = absent despite reinforcement
1 = present only with reinforcement
2 = normal
3 = increased but normal
4 = markedly hyperactive, with clonus
Heel
to toe walking-
Compression of S1 S2 nerve roots
make toe walking painful while that of L5 make heel walking painful.
Power of upper and lower limbs
·
Grade 0: No
contraction or muscle movement
·
Grade 1: Trace of
contraction, but no movement at the joint
·
Grade 2: Movement at
the joint with gravity eliminated
·
Grade 3: Movement
against gravity, but not against added resistance
·
Grade 4: Movement
against external resistance, but less than normal
·
Grade 5: Normal
strength
Modified Medical
Research Council Scale for measuring hand muscles
Grade 5: full active range of motion & Normal muscle
resistance
Grade 4: full active range of motion & Reduced muscle
resistance
Grade 3: full active range of motion & No muscle resistance
Grade 2: Reduced active range of motion & No muscle resistance
Grade 1: No active range of motion & Palpable muscle
contraction only
Grade 0: No active range of motion & No palpable muscle
contraction